ALARA Newsletter - Issue 27 - September 2010
A. Almén, A. Schmitt-Hannig, C. Schieber, P. Vock, S. Christofides, G. Paulo, F. Vanhavere, A. Franck, W. Leitz
One of the major aims of the European Medical ALARA Network (EMAN) project is the creation of a sustainable network: well known by all stakeholders with interest in the application of the ALARA principle in the medical sector; a network that will contribute to achieving and maintaining a good safety culture in this sector.
Work Package 5 (WP5) deals with the methodology for creating this network. The following specific tasks related to these objectives were assigned to WP5:
- To establish cooperation with other networks and make use of their experience,
- To examine different communication strategies in connection to networking,
- To identify success factors for networking and implement these in the continuous development of EMAN,
- To systematically identify and review the roles of the different stakeholders at national and EU levels.
This paper summarises the results of a WP 5 questionnaire addressed to other networks in radiation protection and the implications of these findings for the future work of EMAN.
Questionnaire to European networks related to radiation protection
A number of networks related to the work of EMAN has been explored, either by electronic correspondence, personal communication or by investigating the documentation available on their websites. The following questions were addressed to these networks:
- When did the network start?
- What are the mission and vision of the network?
- Have the mission and vision changed over time, if yes, in what way?
- How large is the network and approximately how many persons are reached?
- In which way is the network organized? (official membership, who is entitled to join, is there a steering board or a committee?)
- How does the network communicate internally? (website, e-meetings, etc.)
- How does the network communicate with communities outside the network? (newsletters, conferences, etc.)
- What are the main products of the network and for who is that of concern? (decision makers, professionals, etc.)
- How is the network financed? (fee, support from outside organizations, advertisements)
- How is the website maintained?
- EAN - European ALARA Network,
- RECAN - Regional European and Central Asian ALARA Network,
- ERPAN - European Radiation Protection Authority Network,
- EUTERP - European Platform on Training and Education in Radiation Protection,
- ENETRAP - European Network on Education and Training in Radiological Protection,
- EURADOS - European Dosimetry Group,
- EUnetHTA - European Network for Health Technology Assessment.
All networks have essentially the same structure for management, similar to that of the present EMAN project. It is a project structure, with a steering group managing the network and working groups performing specific activities. The steering group consists of designated representatives from all or part of the organisations/countries engaged. The number of organisations varies between 10 and 60. For some of the networks the coordinator organisation changes over time. The total number of persons directly or indirectly involved in the network was difficult to assess.
The members of these networks consist mostly of representatives from the organisations represented in the steering group. The members in working groups performing specific actions or tasks are also mostly delegates from these organisations. An important task for all networks is to involve persons outside the core organisations to take part in activities conducted by the network.
Recommendations and guidance documents are the main products of some of the networks. One of the most important target groups for these networks are decision makers. One interesting observation is that decision makers are sometimes part of the network. Some networks have the role of policymakers, other networks perform research. The products of the latter are shared in the research community. Many of the networks use workshops as a tool to disseminate results. It could be interesting to further investigate what impact those type of activities had, for example on guidelines, policies or regulations (at the European or national levels).
All networks, but one, have their own website. The main role of most of these websites is to inform about network activities. In many cases the layout is controlled by project structure and working packages rather than by different topics. One can consider these websites rather conventional with respect to their structures and content. It could be interesting to further investigate how newer communications tools are used or could be used in networking. All networks, not directly supported by the EC or IAEA, have member fees, paid by the member organisations. It is interesting that all networks but one were originally supported by the EC.
In some cases the fee is so high that there is certainly an incentive for each member organisation to monitor the effectiveness of the network, and evaluate whether there is a net benefit for that member organisation. It could be interesting to further investigate, the issue of independence. Specifically to address the issue on how members working in a network can be independent from their own organisation.
Key elements for the success of a network
Through different sources, e.g. personal communication and conference presentations, some key elements for the success of a network could be identified. The possible consequences for the EMAN projected are, to some extent, included.
Management and size of network
The constraints and limits of a network have to be defined during the development stage. For instance the number of members in the network, both from organisations and individuals, should be considered. It could be difficult to provide good service to all members if this number is too high. On the other hand, if it is too low the attraction of the network for all the stakeholders will be reduced and hence their engagement will decline. It should also be clear for all members which services and products can be expected from the network and which cannot.
Good management is important. The network coordinators have to be competent, available, welcoming, approachable and enthusiastic. Good communication skills are crucial and a communication plan will support and facilitate the work of the network.
Successful networks seem to be more flexible than other types of organizations and institutions. When no permission has to be requested or formal rules have to be followed, it is easier to initiate new topics, start up new working groups and to involve people from new stakeholders. The success depends on finding the right type of committed stakeholders that are involved in a topic and bringing them together. The members should come from different backgrounds, different countries and with different experiences. This will favour solutions that will take care of all dimensions of a problem and will therefore be easier to implement into daily practice. Such solutions will be more likely to succeed and be sustainable.
The EMAN network, in order to accomplish the above mentioned success factor should develop a strategy to implement the ideas and expectations of the stakeholders in the network concept, taking into account the different cultural aspects. For the persons responsible for the management of the network, a profile should be established addressing both hard (education, experience) and soft (enthusiasm, engagement, social competence) qualifications, in other words persons that could act as an engine for the network.
Members
Enthusiastic and committed members with communication skills are crucial for a network to be successful. These individuals can discuss real problems encountered in their daily life with others and try to find appropriate solutions. Enthusiastic and committed people are found more frequently in networks providing bottom up actions, such as workshops, group work, web forums and panels, rather than in networks providing top-down actions such as databases and formal tools. Therefore, the network should encourage personal links that can build bridges between organisations. It should provide opportunities for individuals to meet face to face rather than via formal institution channels. When there are no formal rules to follow, many direct links will be introduced that give an opportunity to individuals to express their needs and listen to each other.
EMAN might have different types of members: individuals, but also organisations represented by designated persons. Their involvement and contribution to EMAN might thus differ notably according to the available time they might be able to give to the network functioning or activities. To foster their involvement in the network and their active participation in the future network activities, specific attention will have to be given to the identification of their expectations regarding the network products.
Tasks and products
Before starting a network, its objectives should be defined, and the degree of achieving these objectives should be measurable. A statement of vision and mission should be formulated for guiding the development of the network. Possible products and tasks that are in accordance with these guidelines should be elaborated. The products of the network must be of high quality and focused on practical issues. The network needs to meet the expectations of its members and stakeholders. People are busy and will only continue to participate if they have a benefit.
The EMAN project has to identify the potential market and customers, both inside and outside the network, for its products. The elaboration by the Steering Committee (SC) of a strategic plan covering the medium term (e.g. 3 years) might then help to formalise the objectives of the network according to the members' expectations, and the work programme adopted to reach these objectives. Finally, the SC should, on a regularly basis, check the quality of the products and assess the impact of the networks products on the daily work in the medical environment.
Communication and tools
A network needs to communicate in an efficient way. It must reach relevant stakeholders using the right information and dissemination channels. The message must be delivered in an understandable format. The network needs to be visible and should give status and recognition to its members. People should feel a part of something important and that their efforts are worthwhile. Well-established communication channels will be one factor that may contribute to this.
In this field, the EMAN project will identify the communication channels available (web sites, reports, symposiums, dissemination of information through other networks, publication of guidelines, etc). Information channels will then be selected, with the aim of reaching the target audience in an effective way. The network should consider using channels suitable for each different kind of stakeholder and not to produce one product for all.
It is important to recognize that web-networks and high quality websites are factors for success. Communication between members is also a critical factor. For the time interval between face-to-face meetings, a communication channel strategy must be developed. Web based technology could be one solution for communication between members, most likely contributing to the success of the network.
Financing and integrity
As stated previously, all networks need a minimum amount of financial resources to be able to stay in business in the long term. Preferably financial revenues are created through its own core business by developing its own capacity in this respect. Whatever type of financial scheme will be used (fee from all members, fee from specific organisations, working time allocated to members of specific organisation, a mixture of various schemes etc) care has to be given to its durability and its adequacy to the network objectives and work programme.
In order to accomplish this success factor the EMAN network should work on a policy statement on how different organisations can contribute to finance the network, how individuals from these organisations can participate in the development of the network products as well as other potential financial participation of individual members. The potential administrative structure managing the network should be examined.
Uniqueness
When creating a network, duplication with other networks should be avoided. The network must be unique and represent added value. When there are other networks dealing with similar topics, the new network has to create links with these networks, creating synergies with them and concentrate its work on those items that were identified as not being addressed in the other networks.
To accomplish this success factor the EMAN network should have members that work in hospitals or with good connection to hospital staff. This will be unique for EMAN since this is not the case with existing and related networks. However, this is not the only unique factor: the potential inclusion of manufacturers, hospital managers and patients organisations as well as the objectives, tasks and products are unique to EMAN as well.
Demonstration of efficiency
It is important for a network to show efficiency, to be up-to-date and to present new topics and discussion issues as well as feedback from practical experiences to members, stakeholders and others on a regular basis. The way new experiences are communicated is important, and this should be decided beforehand and stated in a communication and dissemination plan. The communication must be accurate, focussed on real and practical problems, of high quality and released with a timing that will give maximum impact.
The EMAN network will have to create a communication plan, which could be part of the strategic plan proposed earlier, presenting its strategy to communicate with interested parties as well as the mechanisms which will be implemented to monitor its level of success, efficiency and impact.
Possible strategies for EMAN
The analysis of other networks and elaboration of success factors presented above will support the EMAN project in creating its network. However, no decision about the structure of EMAN has yet been taken. The question about what role EMAN should play in the health care environment and in the radiological protection community will have to be further discussed. The outcomes of these discussions will very much influence the network structure.
The project has to decide on the management and size of the network. It should be anticipated that at the beginning of the life of EMAN a strong management is needed, and should be developed on a plan-do-check-act model. The network should work heavily on communication both internally and externally in order to create the identity of the network. Collaboration with persons and organisations should be established before EMAN goes live and should continue throughout its lifetime. At the beginning, the size of the network should not be too large. One suggestion is to keep the number of members to approximately the number of participants in the present project, and try to keep at least some of these members of the project engaged in the beginning of the life of EMAN.
Tasks and products are very important for the network. There is a need to work continuously on this topic during the whole duration of the project so that when the project is finished clear and specific tasks and products are identified. One strategy is to have mechanisms ensuring that the EMAN products are easily identified. In this way the use of the products is referable, the identity of EMAN is strengthened and the efficiency will be evaluated more easily.
Communication and tools are important and any kind of obstacles when using modern communications tools must be avoided. The tools should be usable in a professional setting and this requires special effort that is somewhat different than for social networks. This has to be acknowledged. One tool is the website and the EMAN project will have to carefully think about the structure of the network website. This structure could be perhaps modified in the next project period to be different than the current project structure.
Finding financing and at the same time maintaining integrity is not easy. If financing is regulated by over-stringent policies this could be a problem. The EMAN project will discuss and formulate policies around financing for the network.
Further issues to be studied
The issues discussed above have to be further elaborated. Some key questions need to be answered:
- What is the EMAN added value to the health care environment and radiation protection community?
- How should EMAN interact and complement other networks?
- What are the specifics of EMAN in terms of goals, products, membership?
- With which networks should EMAN interact?
What kind of activities should be conducted by EMAN?
- Are the main objectives: to identify problems, to advocate or to find solutions to problems?
Please have a look at our webpage: http://www.eman-network.eu and send your opinion, ideas, comments to This email address is being protected from spambots. You need JavaScript enabled to view it.This email address is being protected from spambots. You need JavaScript enabled to view it.
Thank you!
Extracts from the IRPA website
Helsinki hosted the third European IRPA Regional Congress during the week of 14 June 2010. The Congress attracted 850 participants from 44 countries. There were 157 oral presentations and 351 posters. The program featured a wide range of topics and refresher courses. A summary of the Congress sessions can be viewed and downloaded from the IRPA website (http://www.irpa.net - see Publications section).
Special focus on the EAN presentation (by Annemarie Schmitt-Hannig (BfS)
The presentation of the European ALARA Network has got a lot of interest, in particular by International Organisations such as IRPA and WHO, who expressed great interest to be involved in EAN activities in the future and offered EAN to use their official distribution channels for disseminating information on ALARA. The presentation can be downloaded from the EAN webpage (http://www.eu-alara.net - see EAN Documents and Publications section).
Brief summary of the International Organisations Forum held during the Regional Congress
The Forum was organised and chaired by Renate Czarwinski from IAEA as part of the Congress Programme (Plenary Session) to review the activities of the International Organizations (EC, IAEA, ICRP, ICRU, ILO, NEA/CRPPH, UNSCEAR, WHO) in radiation protection and conduct a roundtable discussion, moderated by Jacques Lochard (CEPN, France), on the future needs and challenges. The various contributions can be summarized as follows:
- The general challenges facing radiation protection professionals for the coming decades are:
- continuous and rapid increase of medical exposures,
- increasing concern about natural exposures (NORM and radon),
- maintenance of vigilance and good records within the nuclear fuel cycle for both the aging existing installations, and the numerous new installations to be built in the near future, particularly as exposure to maintenance and transient workers are concerned, and
- pursuit of research on low dose radiation effects.
In discussing the need for low dose radiation effects, it was noted that it is necessary to maintain a balance between epidemiological and radiobiological research because the two disciplines are indispensable for establishing sound and effective radiation protection principles.
- More rapid developments related to radiation effects on the lens of the eye, radiation induced vascular effects, protection of the environment from radioactive releases and residues, and attributable risk to radiation are needed to make proper decisions in the coming years.
- Stakeholder involvement is now recognized by all organisations as an effective process to enhance the quality of radiation protection. Efforts should be developed to improve the engagement of stakeholders in the medical field and in existing exposure situations in particular for protection against radon exposure.
- International and professional organizations involved in the global organization of radiation protection must pursue their cooperation for the development of a universal and effective system of radiation protection and take into account the raising role of international networks of authorities, practitioners and operators.
Figure 1. The 4 pillars of the global organisation of radiation protection as presented by ICRP and UNSCEAR Figure taken from W. Weiss, Future direction of the works of UNSCEAR, 3rd European IRPA Congress - International Organisations Forum, 14-18 June 2010, Helsinki (Finland)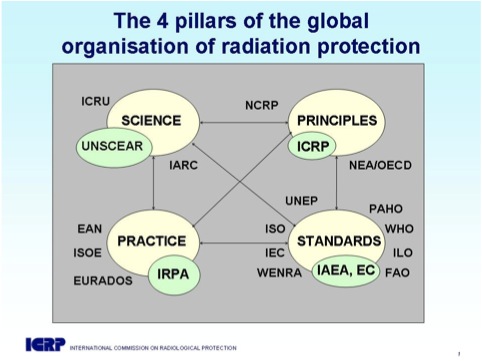
E.G. Friberg, A. Widmark, M. Solberg, T. Wøhni, G. Saxebøl
Section for Dosimtery and Medical Applications, Norwegian Radiation Protection Authority (NRPA), Norway
Introduction
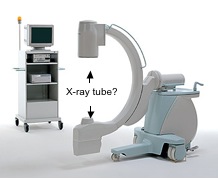
C-arms are a common tool in many interventional and surgical procedures performed outside radiological departments. Common for these procedures is that the C-arm often is operated by physicians without any formal education and training in radiation protection. Modern C-arms have now become highly technically advanced, are used in more and more complex and time consuming procedures and have the potential to deliver high patient doses if operated by unskilled persons. To overcome this problem the Medical Exposure Directive (MED) states in article 7 that radiation protection should be implemented in the basic education for physicians [1]. Norway, as a non-member of the European Union, has not implemented this requirement and radiation protection is practically absent in the basic curriculum of Norwegian medical schools. Our national radiation protection regulation from 2004 states however, that all Hospital Trusts (HT) are obliged to ensure that all personnel involved in radiological examinations have sufficient qualifications and skills in radiation protection [2]. In addition, all HTs must be authorized by the Norwegian Radiation Protection Authority (NRPA) in order to use advanced X-ray equipment for medical purposes. During the authorization process, 54% of the HTs reported inadequate skills in radiation protection among personnel involved in radiological examinations at their local hospitals. The lack of skills in radiation protection was mainly associated with physicians and nurses who were involved in the use of mobile C-arms outside the radiological departments. Finally all HTs confirmed that they had an operating system to ensure that all personnel involved in radiological examinations have sufficient qualifications and skills in radiation protection. The aim of this work was to verify through inspections whether the HTs self-declared compliance regarding training and skills in radiation protection were sufficient or not.

Material and method
The public health care system in Norway is administrated under the Ministry of Health and Care Services. There are approximately 70 public hospitals organized in 21 Hospital Trusts (HT) located under four regional Health Authorities (HA). The NRPA carried out inspections at 52% of all HTs during the year 2008 and 2009. HTs from all regional HAs were included, covering a total of 26% of all the Norwegian public hospitals. The inspections were a direct follow-up of the authorization given to the HTs, with special focus on education and training in radiation protection outside the radiological department. The inspections were carried out as quality system audits, based on document reviews, interviews, on-site inspections and verifications. The HTs local procedures for education and training in radiation protection were reviewed in advance of the inspection. On-site interviews included staff having personnel management and physicians and nurses who were involved in X-ray guided procedures using C-arms. To verify if all involved staff had received training in radiation protection, spot checks of the departments documentation of training were asked for and reviewed.
Results
Procedures for education and training in radiation protection were received from only 64% of the inspected HTs. A review of the procedures indicated that the responsibility for staff involved in X-ray guided procedures was placed on the department heads. All procedures covered regular training in general radiation protection and equipment specific training, including requirements for records of training courses, preferably by signed lists of attendance. Interviews with the department heads revealed that many of them were unaware of their responsibility, some were also unfamiliar with the existence of the procedure in general. A clear distinction between the levels of awareness in radiation protection was observed between nurses and physicians, nurses having the highest level of awareness. Most HTs did not have a systematic approach for education and training in radiation protection. Courses in radiation protection were occasionally held by the radiation protection officer or a medical physicist. The level of attendance on these courses varied between the different professionals (physicians and nurses), departments and hospitals within each HT. Existing systems for documentation of education and training (if any) were highly insufficient at all HTs.
Interviews also revealed some serious lack of skills in radiation protection. Typical examples were: unable to identify the X-ray tube from the image intensifier of the C-arm, inadequate knowledge of the operating consol, no knowledge of the three cardinal principles for staff protection (time, distance and shielding), no deliberate use of collimation and/or pulsed fluoroscopy, and total lack of knowledge about patient doses and risks. In many HTs nurses assisted the physicians by operating the C-arm console. For those cases it was not uncommon to just switch on the X-ray unit and start to fluoroscopy regardless of the default exposure settings on the consol.
The inspections performed by NRPA concluded that 91% of the inspected HTs had non-conformities with the requirements regarding skills and training in radiation protection. This finding makes the HTs self -eclared compliances with the regulation highly questionable.
Discussion and conclusion
The lack of skills in radiation protection among personnel outside radiological departments is clearly not a fiction. The main reason for this is that most HTs had an insufficient system for systematic and frequent education and training in radiation protection. Also the fact that responsible persons were unaware their responsibilities and a general lack of involvement and focus on radiation protection outside radiological departments have to be considered. The lack of knowledge about doses and risks among leaders often tends to unconsciously undermine the importance of radiation protection. As a consequence, radiation protection is often ignored or not prioritized, even though the responsibility is clearly defined.
With modern C-arms becoming more and more complex with the possibility to give high patient doses if operated by unskilled persons, the observations from Norwegian hospitals give rise to concern. There is an urgent need for increasing the knowledge of patient doses and risks among physicians and nurses. The most efficient way to overcome this situation is by introducing radiation protection in the basic education of physicians as stated in the MED. In the short term, focus should be on developing functional systems for education and training in radiation protection locally at each HT and introducing personal driving licenses for operating C-arms. Finally, the biggest challenge is to overcome the bad attitude towards radiation protection present among some physicians. Teaching some dos and donts can have a tremendously impact on patient doses, especially if competence in radiation protection is totally absent [3]. To conclude, there is a common responsibility of the community to improve the operators skills in radiation protection and in this way try to prevent radiation induced hazards caused by malpractice.
References
[1] Council Directive 97/43/EURATOM on health protection of individuals against the dangers of ionising radiation in relation to medical exposure. Official Journal L-180, 09.07.97, p. 22-27.
[2] Regulations No. 1362 of 21 November on Radiation Protection and Use of Radiation (Radiation Protection Regulations). Oslo, 2003. http://www.nrpa.no/archive/Internett/Publikasjoner/Annet/act_eng.pdf (17.02.2010).
[3] Widmark A, Friberg EG. How dos and donts can be of significant importance in radiation protection training. In: 4th International Conference on Education and Training in Radiological Protection, Lisbon 2009. ETRAP 2009 transactions. Poster session. Brussel: European Nuclear Society, 2009. http://www.euronuclear.org/events/etrap/transactions/ETRAP09-poster.pdf (17.02.2010)